I am confused with the way metformin been presented as damaging to muscle mitochondrial function.
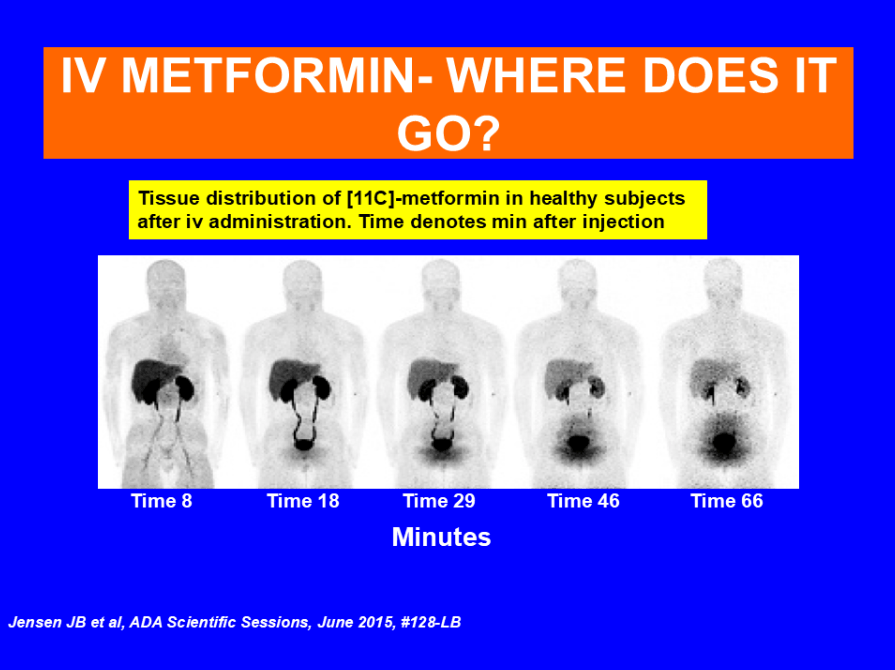
From the data I have it is not affecting muscles mitochondria and works only on the liver in humans. Can also being studied for sarcopenia as a new indication.
Exploring the protective effect of metformin against sarcopenia: insights from cohort studies and genetics – PMC
2015 American Diabetes Association’s Scientific Sessions
And this are excerpts from the person with the most experience with Metformin Ralph A. Defronzo, MD (Professor of Medicine, Chief, Diabetes Division, Deputy Director, Texas Diabetes Institute) during his discussion with Peter Attia, MD:
- Everybody wants to know if metformin is geroprotective.
Remind people, metformin inhibits complex I of the electron transport chain
- This is still controversial
- In high doses, it does for sure
- In the doses you give metformin, it’s somewhat equivocal
Is the belief that metformin’s efficacy in diabetes is through reducing hepatic glucose output?
What’s the mechanism by which it reduces hepatic glucose output?
- Inhibiting the mitochondrial chain and inhibiting gluconeogenesis
- For sure it inhibits gluconeogenesis
- Metformin gets in the cells through the organic cation transporter
⇒ The organic cation transporter doesn’t exist in muscle; it can’t possibly be an insulin sensitizer in muscle (you’re asking the drug to do something that’s impossible)
- Metformin enters cells using the organic cation transporter, and it does not exist in skeletal muscle or cardiac muscle ‒ so metformin cannot get into those tissues
- A rare complication that can occur when you have very low GFR and/or very, very high doses: lactic acidosis
- Metformin is excreted by the kidney.
Can you please clarify your opinion and approach.
 .
.