Forum Replies Created
-
AuthorPosts
-
Has she had any labs for autoimmune process. Thyroid antibodies, ANA and secondary antibodies for autoimmune conversion after covid (not uncommon). At least add back quercetin and SPM https://17fwxf1trr45xut7r3i2d4ya-wpengine.netdna-ssl.com/wp-content/uploads/2018/06/TimesStyleArticleREVISEDv6_2018.pdf
Lab interpretation: https://test.mayocliniclabs.com/it-mmfiles/Autoimmune_Disease_Testing_Algorithm.pdf
Covid/autoimmune: https://pubmed.ncbi.nlm.nih.gov/33332890/
May consider adding back hydroxychloroquine if positive autoimmune panel. I also follow endothelial dysfunction parameters, MPO, LP-PLA2, Fibrinogen Ag and if + use Nattokinase
Natural fibrinolytic: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5372539/
Thinks of post covid as a systemic autoimmune dysregulation chronic inflammatory syndrome, CIRS etc. If unilateral edema evaluate for thrombosis .
For peptides: yes if fibrosis markers present TB4 https://pubmed.ncbi.nlm.nih.gov/?term=Thymosin%20beta%204%20fibrosis
melanotan II https://pubmed.ncbi.nlm.nih.gov/?term=Melanocyte+stimulating+hormone+anti+inflammatory
Hope that gives you some other things to work with
Carl
Maybe this is what the pt was reviewing: https://pubmed.ncbi.nlm.nih.gov/30971892/
more history would be useful regarding alcohol, drugs (recreational or prescription). Also PTSD for whatever trigger including chronic pain. I would consider LDN for endorphin modulation. If you have access to it then Cerebrolysin, lots of info on it for for depression post stroke/TBI and I have foud it very effective for other forms of depression . I have not seen anxiety/depression myself manifest in the 100’s of patients i have used TB4 with but of course that is doesnt mean it couldnt happen.
February 15, 2022 at 6:11 pm in reply to: nontuberculous mycobacteria with Mycobacterium avium complex #31556I have a case study regarding MAI/MAC. Patient followed serially for this by pulmonary with CT and plain chest films. No antibiotics. I placed her on TA-1 in 2018 and over a 4-5 month period before her scheduled pulmonary follow up. The scans had “improved dramatically” according to pulmonary in that interim and they had no other explanation or new intervention during that period. The patient is a retired ICU nurse and was very consistent with TA-1 just 3 days per week and daily if any exacerbations. I only have the one case to report. Excellent response clinically with improved respiratory capacity and imaging. She “will never go off Thymosin alpha” based on how she now feels. Now I would probably start with a higher daily dose at least 25u until improvement before considering tapering bellow daily administration
Carl
That’s very unfortunate. If she has lost muscle tissue (looks like it in the photo) then Peg-MGF 10u up to daily or at least 3-4 days per week. If she can I would increase the BPC/TB4 to 15u twice daily. Exosome topically or IV. Collagen support nutritionally.
If possible I try to recover natural Testosterone production with managing underlying medical/metabolic issues and use of KISSPEPTIN, and or enclomiphene or similar products. If this is not practical, appropriate or ineffective I use IM / SQ for those patients requiring replacement Testosterone. For IM use of a cypionate, or enthanate oil once weekly minimum frequency or twice weekly IM to provide the smoothest coverage. Also if the patient does not want IM delivery for whatever reason I will take the weekly dose divided by 7 and dispense SQ with excellent results. Every 2 week dosing is not appropriate considering the 1/2 life of these products.
Carl
Pentosan polysulfate for inflammatory component. Maximizing the LL37 and TA-1 yes. Another perspective from 30yrs of primary care experience regarding tooth pain/need for root canal/dental “infection” , is to keep in your differential that many of these “syndromes” are consistent with a dermatomal unilateral distribution (think shingles, herpes) and manage with that in mind with appropriate anti-viral therapy. Trigeminal V2(maxillary) upper tooth, V3(mandibular) lower tooth.
I do not market/claim essentially anything regarding peptides at all. Peptides are a tool we use with patients on an individual basis. LDN has fairly robust anecdotal use in the traditional and integrative space for fertility and published literature in the narcotic addicted mother so you should be fairly safe there. Anecdotally I have lost count of the female patients who have begun cycling/ovulating more consistently in the perimenopausal age range and younger when GHRP/GHRP was introduced. A few of them have conceived after GHRH/GHRP after they had given up on conception (all were very happy). I now notify all cycling/perimenopausal that use of growth hormone secretagogues by enhancing ovulatory efficiency etc. will possible increase the potential conception and to consent to use in that context. I do think that the reproductive OB’s have published on use of GH support prior to egg harvest etc. Also a lot of literature on GHRELIN agonists and reproductive health in the context of metabolic optimization. It does make sense with the pleiotropic impact of GH on the endocrine system as a whole, receptor sensitivity peripherally. I would never market or claim this though but you definitely should be aware of its impacts in this arena.
https://pubmed.ncbi.nlm.nih.gov/?term=Ghelin++infertility
https://pubmed.ncbi.nlm.nih.gov/?term=Growth+hormone+fertility
August 13, 2021 at 6:59 pm in reply to: Advice for performance optimization for an 18 yo Lacrosse player #30986It would be helpful to know if the athletes in question are under WADA review to help with options. Working with circadian rhythm optimization, use of a wearable to ensure sleep efficiency (OURA ring etc. ) to dial in recovery sleep. Many over trained athletes will have hypothalamic /pituitary /gonadal (HPG) axis dysfunciton that may need to be recovered with rest, breaks from training ( They usually look great externally but their labs look awful). CJC/ipa, kisspeptin, etc. can be used short term to combined with rest, training breaks to recovery normal HPG funciton.
Carl
Testosterone in prostate cancer. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4647137/
Hypothalamic/pituitary/gonadal axis. https://www.ncbi.nlm.nih.gov/core/lw/2.0/html/tileshop_pmc/tileshop_pmc_inline.html?title=Click%20on%20image%20to%20zoom&p=PMC3&id=2948422_ijcp0064-0682-f1.jpg
SARMS and BPH. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2098692/
T replacement vs Clomiphene https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5508437/
With LH in normal range but low for his suboptimal T levels clomiphene, enclomiphene may not have a significant impact. It would be helpful to evaluate his estradiol/estrone levels as they will suppress LH response to low T levels LH, FSH, DHT levels (blood) and alpha reductase / aromatase assessment would be useful (DUTCH) test to get a more complete picture of to determine whether T replacement, hypothalamic (kisspeptin) / pituitary (clomiphene), estrogen detox support, or possible SARMS would be the most apporpriate management In any case inform, consent, document, correspondence with urologist should be done for risk management purposes which ever path is choosen
CJC/IPA will enhance T receptors peripherally and overall hormone funciton pletropically and I often use this first before initiating direct T modulation by any of the above then reevaluate labs mentioned and determine best approach.
GH pleitropic effects https://www.mdpi.com/ijms/ijms-19-00290/article_deploy/html/images/ijms-19-00290-g001.png
Carl
TA-1 + LL37. Start both together, stop LL37 when acute inflammatory pustular lesions resolved. TA-1 may need stay on sometime until underlying metabolic/hormonal/nutrition issues addressed. Reinitiate LL37 early for exacerbations. With the same combo general cystic inflammatory acne has responded very well in several patients as well. I am not injecting into any lesions directly but just regular SQ for systemic effect. I have one college level athlete that has complete remission of severe persistent HS with this combo
Carl
I have not used and do not plan to use peptide sciences and have not had any direct contact with them or any online vendor. Here is a link from peptide sciences regarding their “terms and conditions”.
https://www.peptidesciences.com/terms
Read for yourself but below is a some of the page content. I am not trusting patients health/outcomes/my license/regulatory oversight risk etc. by recommending or managing use of products from these types of companies. They may have great equipment, policies, procedures and produce a great product that is completely equivalent to a traditionally compounded product, but would really have no leg to stand on from a risk management or compliance standpoint using or recommending these products. They are basically washing their hands of any liability regarding use outside of their listed guidelines. If they have disclaimed any liability very clearly then it would likely fall to the provider involved in the recommendations or management of the use of said products.
“PeptideSciences.com products are intended for laboratory IN-VITRO RESEARCH PURPOSES ONLY– NOT FOR HUMAN or ANIMAL USE or CONSUMPTION of any kind and are not to be used for any other purposes, including but not limited to food and/or drugs, medical devices, vitro diagnostic purpose, or for commercial purposes. The purchaser agrees that the products have not been sterilized or tested by PeptideSciences.com for safety and efficacy in food, drug, medical device, cosmetic, commercial or any other use. The purchaser expressly represents and warrants to PeptideSciences.com that the purchaser will properly test, use, manufacture and market any products purchased from PeptideSciences.com and/or materials produced with products purchased from PeptideSciences.com in accordance with the practices of a reliable person who is experienced in the field and in strict compliance with all applicable laws and regulations, now and hereinafter enacted. The purchaser further warrants that any material produced with any product shall not be adulterated or misbranded within the meaning of the Federal Food, Drug, and Cosmetic Act and shall not be materials which may not, under Sections 404, 505, or 512 of the Act, be introduced into interstate commerce.
The purchaser realizes and agrees that, since PeptideSciences.com products are, unless otherwise stated, intended solely for in-vitro research purposes, they may not be on the Toxic Substances Control Act (TSCA) inventory listing. The purchaser assumes responsibility to assure that the products purchased from PeptideSciences.com are approved for use under TSCA, if applicable.
Purchaser has the responsibility to verify the hazards and to conduct any further research necessary to learn the hazards involved in using products purchased from http://www.peptidesciences.com. No products purchased from http://www.peptidesciences.com shall, unless otherwise stated, be considered to be foods, drugs, medical devices or cosmetics. ALL products and services offered are for RESEARCH purposes ONLY. Under NO circumstances shall/should ANY of these materials be used for therapeutic or diagnostic purposes. Peptidesciences.com is NOT liable for ANY damages that may be caused by negligence, abuse, or ANY other unforeseen matter.”
Carl
If inflammation is a concern and especially in that age range you might consider TA-1 for immune modulation for a month or so before introducing GH augmentation. Autophagy promotion with fasting mimicking, intermittent fasting, senomodulation ie rapamycin et al. before tb4 for sure and probably the cjc/ipa.
Using CJC/IPA in a 5 out of 7 day cycle is essentially intermittent use. Approximately one week per month (2 consecutive weekend days per week x 4 weeks = 8 days) there is a “holiday” from use. This should be enough to prevent desensitization. The GHRP component will work against somastatin effect. The point being do not go off for 6 or 8 weeks but just cycle off on weekends.
Carl
I agree with Abid’s excellent post and appreciate the info on VIP in cardiovascular disease. Most common uses of VIP in my practice is for circadian rhythm/shift work disorder patients to help reset the clock. Particularly in my commercial pilot patients who cross many time zones per week. Using intranasal. In this scenario I am not monitoring levels and use is temporary. Our current supplier is PURE for the VIP.
https://www.jneurosci.org/content/34/17/6040
Carl
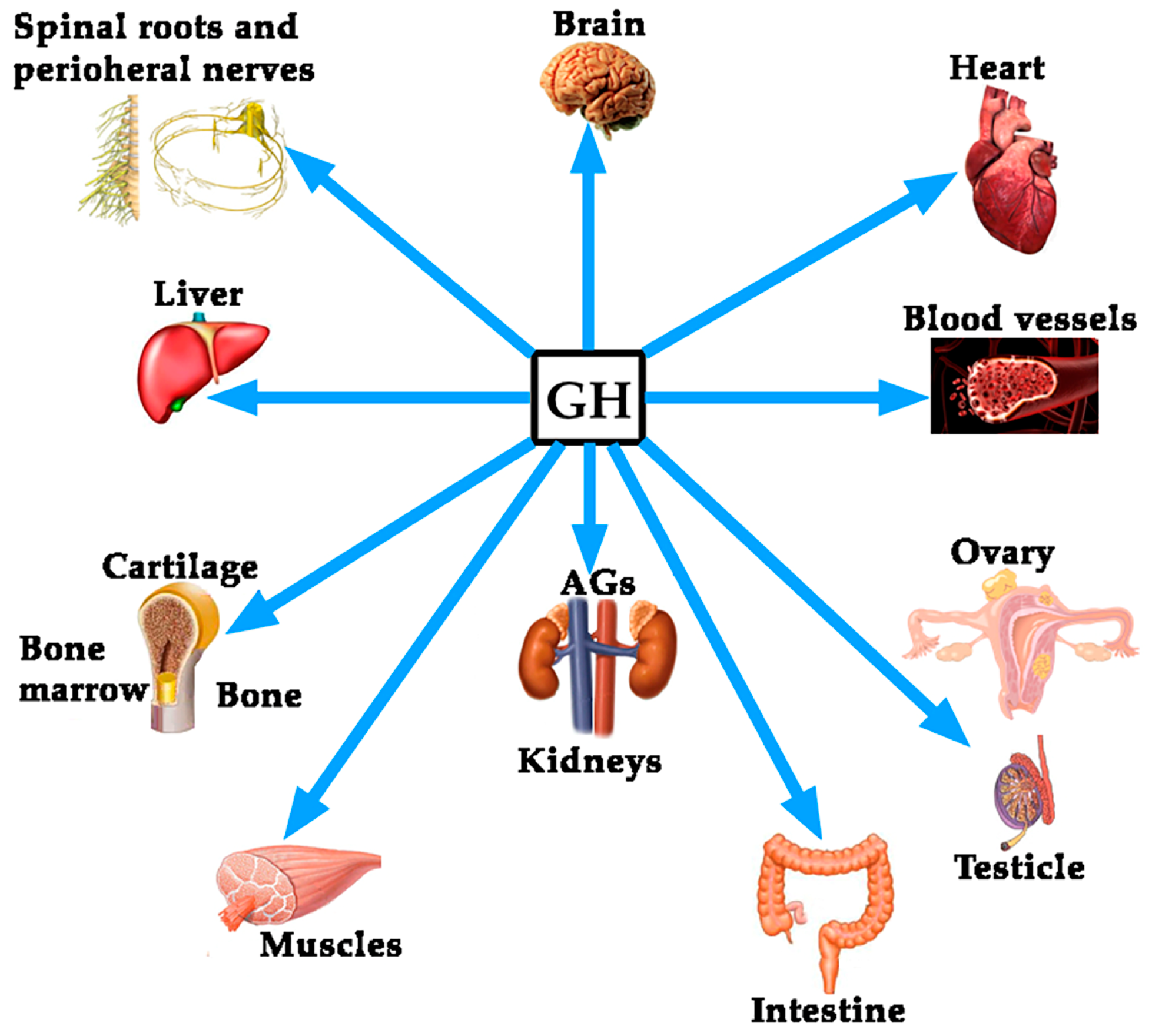
In general support of ideal GH levels (cjc/ipa) in older potential mothers would conceptually be beneficial to overall health celluar efficiency, receptor optimization etc. It does appear in my clinical experience That optimal endogenous sex hormone levels are maintained longer in men and women with consistent use of GH support. see image. Growth hormone. Most of the clinical literature I reviewed was around Growth hormone replacement to augment IVF not natural fertility. Much of infertility is auto/immune, inflammatory so addressing root causes there along with immune modulation with thymosin alpha -1 would make sense. (. it is pregnancy category C as commercial ZADAXIN).
-
AuthorPosts
{kind=link}